
What’s the deal with inverted typhoid?
Maybe it’s just lack of familiarity with other disciplines’ historical documents, but I feel like old medical and biological articles are particularly thick with phrases that are totally opaque now, but were self-evident to the people of the time. Phrases like “inverted typhoid” represent a type of jargon that is specific not just to a certain profession, but to a certain profession at a certain time in history.
* * *
First of all, what’s “typhoid”? Typhoid fever is a disease characterized by fever. There are other symptoms, like distended abdomen, diarrhea, elevated heart rate, “rose spots” on the abdomen, bacilli in the blood, and borborygmus. And positive results from molecular tests that range from the century-old Widal test for agglutinating antibody, to blood levels of liver enzymes. But the fever itself is a major part of the diagnosis.
This free chapter from 1990’s Clinical Methods (published by Butterworth, Boston) gives an overview of the different fevers caused by different diseases. Fever is typically lowest in the morning and highest in the evening, in a healthy person. Many sources say the typical range is between 0.5 and 1 degree Celsius, though this chapter says it can be as high as 1.5°C. Diagnoses based on various fevers can include:
Although not diagnostic, at times fever curves can be suggestive. Hectic fevers, because of wide swings in temperature, are often associated with chills and sweats. This pattern is thought to be very suggestive of an abscess or pyogenic infection such as pyelonephritis and ascending cholangitis, but may also be seen with tuberculosis, hypernephromas, lymphomas, and drug reactions.
…
Relapsing fevers may be seen in rat-bite fever, malaria, cholangitis, infections with Borrelia recurrentis, Hodgkin’s disease (Pel-Ebstein fever), and other neoplasms.
Historically, some diseases are described as having characteristic fever patterns. The double quotidian fever of gonococcal endocarditis has two spikes in a 24-hour period. Fever at 48-hour intervals suggests Plasmodium vivax or P. ovale; 72-hour intervals suggest P. malariae, while P. falciparum often has an unsynchronized intermittent fever.
So, you’ve got relapsing fever, hectic fever, double quotidian fever, and so on. What’s the pattern of typhoid fever? In his 1901 book Typhoid Fever and Typhus Fever, Heinrich Curschmann of the University of Leipzig gives some examples.
* * *
Here’s someone who came down with typhoid when he was recovering from “polyarthritis”, which is why they were already measuring his temperature. In all these graphs, the body temperature was measured once in the morning and once in the evening. Note that this guy starts out with small fluctuations between morning (low) and evening (high), and the difference between morning and evening gets exaggerated when the fever begins.

Here’s the plateau stage of the fever, following the familiar “Wunderlich curve”. The difference between morning and evening continues to grow, even as the temperature itself levels off and gradually decreases.

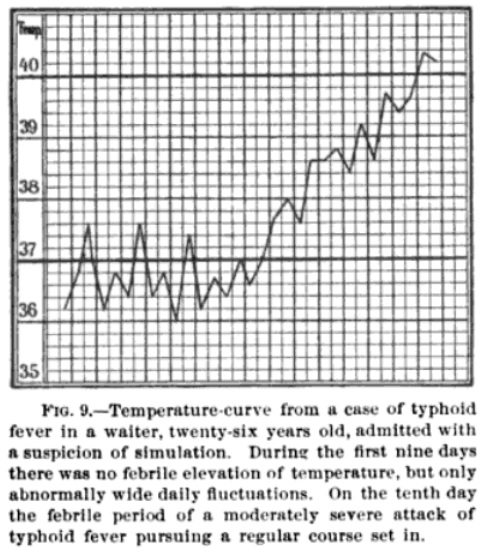
Here’s a guy who was thought to be faking illness but was brought to the hospital anyway. The point of this graph is that in his first week in the hospital he was not showing a particularly high temperature, but the large daily fluctuations should have been a warning sign that he might have typhoid.
The “typhoid” pattern is a large fluctuation between morning temperature (low) and evening temperature (high). The period of low temperature can also be thought of as the “pre-dawn” or “night”, as the nadir is usually around 4 AM. Terms vary.
* * *
Looking at it from that perspective, it makes sense that there would be something called “inverted typhoid”. This term means a pattern in which the fever is highest in the morning, and reaches a low point in the evening.
Here’s some examples.
From John McCaw’s 1914 Diseases of Children:
During the Second Week: The spleen is enlarged and tender, the abdomen is uniformly swollen, and gurgling in the right iliac fossa is present. The bowels may be relaxed, but quite as often they are constipated. Headache subsides, and delirium at night takes its place. The expression is dull, the decubitus dorsal, the cheeks are flushed, and the child is indifferent to its surroundings, but not in any apparent suffering. Thirst is considerable, and the skin is dry. The temperature varies from 101.5°F to 105°F, rising towards evening and falling again in the early morning, but throughout the attack the highest temperature may be recorded in the morning (inverted typhoid).
From the 1913 Journal of the Indiana State Medical Association:
Dr. Bruggeman: Had patient with a deep phlegmon of the palmar fascia which was incised and drained. Perfect recovery from hand. Two weeks later dull pain in right hypochondrium. Urine normal. Blood showed slight leukocytosis. Examination negative. Lowest temperature from 101 to 103; no chill. Temperature is of the inverted typhoid type. Widal negative. Leukocytosis diminished.
From the 1884 Dublin Journal of Medical Science (describing a fever that isn’t necessarily infectious at all):
Temperature in Insanity.— Extended contributions to this subject have recently been made by Bechterew (Archiv für Psychiatrie, Bd. XIII.) and Hebold. Bechterew has taken the temperature of the rectum with all the precautions suggested by Liebermeister. He finds that in the first stage of melancholia the temperature usually remains normal, or may even rise above it. It has been observed as high as 104°F. By melancholia Bechterew evidently means all cases with delusions of persecution and depression. …In the convalescent period the temperature is usually normal. Sometimes the temperature is extremely variable at the outset of this period, and this usually denotes a sudden improvement in the patient’s condition. In the excited or stuporose period an inverted typhoid fever curve is often noticeable.
In 1867’s Notes on Asiatic Cholera, John Charles Peters viewed “inverted cholera” yet another way.
Some physicians believe that cholera is in some strange way mixed up with intermittent and remittent fevers in India in the East; and with typhoid fever in Europe and the West. Others have even gone so far as to describe cholera as an inverted typhoid fever; it commences with profuse discharges, and the latter is apt to end with them; the one has collapse before the fever, and the other afterwards, &c.; the causes of both are said to be similar with the difference of climate only.
Coincidentally, the first convenient clinical thermometer was manufactured in 1867! So Dr. Peters was writing this in a world before typhoid was known to have an easily-measured daily fever cycle. Even then, it was a disease with a standard pattern of symptoms to which other diseases could be compared and contrasted.
* * *
Okay. “Inverted typhoid” is a symptom, that is not necessarily indicative of typhoid, or even of infection. It means high fever in the morning, and not so high in the evening.
But when you look into “inverted typhoid”, the most significant article on the subject is a piece in the 1898 Medical Record, by Max Goltman of the Shelby County Poor and Insane Asylum, Memphis, Tennessee. For more about the Glasgow-born Dr. Goltman, see the Jewish Historical Society of Memphis and the Mid-South .
.
Dr. Goltman’s definition of “inverted typhoid” is different.
On September 25, 1897, I was called to see Arthur Z—–, thirteen years of age, white. He was born and brought up in Memphis, and was bright, exceedingly energetic, and of a very nervous temperament. …
He had been indisposed, more or less, for about two weeks prior to my first visit, complaining of throbbing headaches, which were worse in the afternoon and after exercise; and there were loss of appetite, lassitude, drowsiness, disturbed sleep, constipation, and feverishness. Being an ardent cyclist, he made frequent trips far into the country in the hot sun. He recollected having partaken, on several such occasions, of both milk and water at a roadhouse where there had been sickness in the family for some time.
I diagnosed malaria, and prescribed a saline purge and quinine in three-grain capsules every four hours, an ice cap to the head, and a cool bath. About six hours later I received word that the patient was resting nicely and was nearly, but not quite, free from fever. On September 26th he had another chill, which was of a much milder character than that of the preceding day. The quinine was continued until twenty-four grains were taken. This kept the patient comfortable, but with a temperature ranging from 99° to 101°F until September 29th, when he had another violent chill, followed in a short time by fever of 104.8°F. On being informed of this, I made an examination of the blood for malaria.
What seemed like a typical case of malaria is not following the normal pattern, so he looks to see if it really is malaria. The parasites are clearly there in the blood cells. But the symptoms keep changing. I’m no doctor, let alone a 19th-century doctor, so I don’t know why he suspected that malaria was “not accounting for the symptoms present”. Maybe the patient was no longer having chills. Anyway, three days after seeing malaria under the microscope, he looked for other pathogens, and the Widal reaction showed clear signs of typhoid.
But the fever didn’t follow the typhoid pattern any more than it followed the malaria pattern. Here’s Goltman’s temperature chart of “inverted typhoid”.

As you can see, Arthur Z—- starts out with a fever. But the “Rose Spots” noted on Day 6, normally found in the plateau stage of typhoid fever, are here accompanied by a decrease in fever, quickly reaching sub-normal temperature. At this point Arthur had probably been switched from quinine to heavy doses of cathartics, with the goal of maximizing bowel movements to get rid of the bacteria.
I [have] discussed the eliminative treatment of typhoid fever very extensively, and urged the adoption of the saline cathartics for the purpose of elimination in preference to anything else. I have no reason to change the opinion then expressed. They are undoubtedly best and safest. The patient may get tired of salts; then, for a day or two, calomel may be substituted in broken doses until the bowels move. A good mixture to employ is a drachm each of Epsom salts, Rochelle salts, and compound licorice syrup, repeated if necessary. Four or five movements a day are desirable. This is my main treatment; everything else is subservient to it.
And indeed, as the patient “got tired of salts”, he replaced the cathartic salts with one dose of strychnine, followed by calomel. This coincides exactly with the body temperature returning to normal. Whether the treatment helped or hurt, who knows. The point is that we have, as Dr. Goltman says in his somewhat flowery conclusion, “an Æsculapian paradox — a fever without fever”. In other words, a case of inverted typhoid.
One more quote.
Gentlemen, we have here for analysis a case of atypical typhoid fever ushered in by the clear-cut paroxysms of a malarial infection, which was demonstrated beyond the shadow of a doubt by microscopic examination of the stained and fresh blood of the patient. More typical organisms I have never seen … Having made such a diagnosis in this case, it was somewhat humiliating to be compelled apparently to recede from my position, and inform the anxious family that they had now to nurse a case of typhoid fever. Dr. Pheemster has, however, told me of a similar instance occurring at St. Joseph’s Hospital, and the literature of the subject teems with similar cases, which, unlike my own, however, are somewhat lacking in scientific data and therefore of doubtful value.
First of all, I highly doubt there was ever a person named “Dr. Pheemster”. That sounds like a Robert Benchley character. Second of all, is it necessary to claim that yours is the only reliable case report ever published? It’s not like you have lots of data either. Just one temperature chart.
Finally, another frequently re-printed study, originally in JAMA, mentioned “inverted typhoid” in passing. This was by Dr. George Boody, recounting a typhoid outbreak at the Iowa State Hospital for the Insane (now the Independence Mental Health Institute). Dr. Boody includes a multi-week fever curve similar to that of Dr. Goltman, indicating that to him the term refers to a case of typhoid that progresses from fever to sub-normal temperature. He doesn’t mention malaria or any other comorbidities, saying simply that “[c]ases of typhoid fever are comparatively quite rare, and the subject is deserving of thorough investigation as often and wherever an epidemic occurs… In these two epidemics it occurred but once in forty-three cases.”
* * *
So, we have “inverted typhoid” meaning a case of typhoid where the fever goes down rather than up, because of malaria. Or it means a case where the fever is high in the morning rather than the evening. Or it means a case that does not involve actual typhoid, just a typhoid-esque fever pattern.
Good thing nobody uses the term anymore! Instead, we use the term “typhus inversus”, which meant the same thing as “inverted typhoid” back in Dr. Goltman’s day. Now “inverted typhoid” has died out, but “typhus inversus” remains.
From Khan Abdul Kalam Azad (2011), Changing trends in pattern of presentation with different types of pyrexia and approach to be made. J Dhaka Med Coll 20(1):1-3 (available here):
A diurnal pattern also known as typhus inversus, is the reverse of normal circadian pattern in which the highest temperature is in the morning. It can be found in miliary TB, hepatic abscesses and endocarditis.
The same definition is in ML Kulkarni (2008), Clinical Methods in Paediatrics: Physical Examination of Children (Jaypee Brothers Medical Publishers, New Delhi), page 61 (partially available here), and in the fourth edition of Moffet’s Pediatric Infectious Diseases: A Problem-oriented Approach (2005) by Fisher, Boyce and Moffet (partially available here).
Calling it “typhus inversus” is less confusing than implying that the person suffering from TB or salmonellosis also has some odd form of typhoid.
But it’s still confusing.








