
The Clinical Research Laboratory: where ophthalmology meets urine
by Mike
That last article had another odd element that warrants further study. No, not Table 1, which lists the counts of Clostridum welchii per gram of dry feces for 30 donors of varying degrees of anonymization (“H.”, “J. J.”, “L. W. R.”, “Mr. L.”, “Mrs. C. H.”, “Irwin H.”, “Gladys H.”). I’m referring to the author’s affiliation.

Clinical Research Laboratory? What’s that?
Probably a branch of the city health department. But wouldn’t “clinical” be more likely part of a hospital?
I had to find out. Now, searching for “Clinical Research Laboratory” “New York” is useless. That is the ultimate generic name. Maybe if it was the Clinical Research Laboratory, Manitowoc, Wisconsin I could find details on this now-defunct facility.
But looking for other papers by George H. Chapman gives the answer.
* * *
Over the 25 years following the 1928 paper which documents him burning his hands on a jar, Chapman shows up again and again in the Journal of Bacteriology, mostly as a single author, mostly suggesting small improvements in how to culture and differentiate common bacteria. If we ignore the ones by a George H. Chapman, M.Sc. who worked at the Massachusetts Agricultural Experiment Station, and the other bacteriological George Chapman at Princeton University, there are still about 40.

There are also a couple in journals other than J. Bacteriol.

Without exception, George H. Chapman is affiliated with the Clinical Research Laboratory. Occasionally co-authors appear, most often from the Lighthouse Eye Clinic of the New York Association for the Blind.
The New York Association for the Blind is an organization that started out as “The Lighthouse” and is now “Lighthouse International”. According to their website, “In 1952, the Lighthouse forged an affiliation with the Ophthalmological Foundation, which became the research arm of the Lighthouse at that time. The Foundation was the first to devote its resources to the research of blindness.”
About half of the Chapman papers have a footnote reading “Aided by grants from the Ophthalmological Foundation, Inc.” Does this mean the “Clinical Research Laboratory” was the laboratory of the Ophthalmological Foundation, which ceased to exist after 1952 when it was folded into the Lighthouse? Is that what happened? And why do I care?
More likely, the Ophthalmological Foundation was what it sounds like, a charitable organization that funded all kinds of research. Searching for “Ophthalmological Foundation Inc” did bring up a bunch of articles that don’t mention George H. Chapman. But for most or all of them, if they don’t include him as an author, they do include Conrad Berens, M.D.

The beginning of Berens’s 5-page obituary in the Transactions of the American Ophthalmological Society
Noted ocular surgeon Berens was apparently quite the fundraiser and organizer. The obituary goes on to credit him with founding or leading a dozen societies, receiving the Chevalier de l’Ordre de la Santé Publique and the Orden al Mérito de Duarte, Sánchez y Mella, and being a consulting ophthalmologist at eleven hospitals including his primary appointment at the New York Eye and Ear Infirmary. He was also Managing Director of The Ophthalmological Foundation, Inc.
The various affiliations on Berens’s papers include:
Department of Research, New York Eye and Ear Infirmary
Department of Motor Anomalies, New York Eye and Ear Infirmary
Orthoptic Training Department, New York Eye and Ear Infirmary
Department of Ophthalmology, New York University Post-Graduate School of Medicine
Department of Research, New York Association for the Blind
So was this the clinical lab of the New York Eye and Ear Infirmary? If so, why not say that?
More from Berens’s obituary:
At the height of his career, Dr. Berens enjoyed one of the most varied practices of ophthalmology in the United States. His patients came from all walks of life and received the same courteous treatment whether rich or poor. At one time, he employed five medical associates and nine ancillary aids to help him with his private work and he usually had one or two visiting ophthalmologists learning his office technique. His assistants were always known as associates and learned early never to discuss diagnosis and treatment in front of the patients.
The Berens Clinic of the New York Eye and Ear Infirmary early became one of the most progressive in the New York area and popularized a general medical survey before operation or treatment was started. He required orthoptic analysis and treatment before surgery for squint and established the first course in orthoptic training at the Infirmary. Through the aid of the Ophthalmic Foundation, Inc. he established the original Department of Research in Ophthalmology at the hospital. His clinic was the first to make use of preoperative bacteriologic tests and sterile gloves in the operating room.
So he had a private practice with a dozen or so staff, and also founded a “Berens Clinic” at the hospital where he did his published research and tried out new devices. This “Berens Clinic” pioneered doing general physicals and bacteriological tests on all patients, on a larger scale than ophthalmologists had done before. Most likely George H. Chapman was essentially an employee of Dr. Conrad Berens, in charge of whatever bacterial tests were needed for all kinds of patients (certainly most of the samples he handled were from regions of the body distant from the eye) from the New York Eye and Ear Infirmary. And in the process of improving his lab’s techniques, he kept careful track of everything and came up with some stuff that could be published.
* * *
Wait. Isn’t there an address after the words “Clinical Research Laboratory” up there? Can’t we look up which hospital or clinic was at that address?
604 Fifth Avenue is actually a well-known building. A well-known, tiny building in Midtown Manhattan, right near Rockefeller Center. It was built in 1925 to house a Childs restaurant. Childs Restaurants was a pioneer in the concept of fast food, and just like today’s fast food chains, they hired top architects to create novel architectural treasures which would house distinctive flagship restaurants. Here’s a 2010 New York Times article by Christopher Gray, spotlighting this exact building and its current status wedged between two much taller and more important architectural treasures.
604 Fifth Avenue, by the way, is far from the New York Eye and Ear Infirmary, which is and was in Lower Manhattan between 14th and 13th Streets. I can’t find a reference to 604 Fifth Avenue containing anything other than a Childs restaurant, a T.G.I. Friday’s, a series of jewelry stores, or the apartment of Mrs. Russell Sage, widow of one of Jay Gould’s plutocratic pals. We could investigate what hospitals were nearby, but that would take forever. So let’s just say the Clinical Research Laboratory, despite its considerable interest in the bacteria of the GI tract, was run by a ophthalmologist and loosely affiliated with the New York Eye and Ear Infirmary.
* * *
As for George H. Chapman, the flood of bacteriological articles stopped in 1952, the same year the Lighthouse and the Ophthalmological Foundation merged. Years later, he reappeared with a 34-page treatise that was presented at the October 1962 meeting of the New York Academy of Sciences’ Division of Microbiology, and published that November in Trans. N.Y. Acad. Sci.
The title is “Microbial origin of the gummy substance of Fujita and Ging”. It’s a weird article, but not weird in the way that the title sounds weird. Basically he takes the established idea that there are probably distinct toxic chemicals in the bodily fluids of people with schizophrenia, and explains that they are signs of bacterial infection.
The substance of Fujita and Ging had been described less than a year earlier, in “Presence of toxic factors in urine from schizophrenic subjects” (Fujita S, Ging NS [1961] Science 134(3491): 1687-1688). The table of contents for that issue of Science is in JSTOR here. At the time Science was mostly editorials, book reviews, and extremely short research “Reports”, plus a couple longer articles. This was one of the Reports, and as such documented a single experiment, in which a series of mice were injected intracranially with extracts of urine from schizophrenic or non-schizophrenic men “who had been kept for at least 4 weeks under controlled conditions” at the Ypsilanti State Hospital. Looking for signs of schizophrenia in bodily fluids was a frequent topic of study, though urine was not looked at as often as blood; Fujita and Ging explain that they are extending into mice the studies of Wada and Gibson, who did a lot of experiments of this sort on monkeys and cats in a 1959 paper that appeared in the very last issue of AMA Archives of Neurology & Psychiatry.
Fujita and Ging were part of the research team of the University of Michigan’s legendary neuroscientist Ralph W. Gerard. Fujita was visiting from the University of Sapporo, and did eventually publish a follow-up paper on what the chemicals might be in the schizophrenic urine. But for me the trail ends there, since it’s in Japanese.
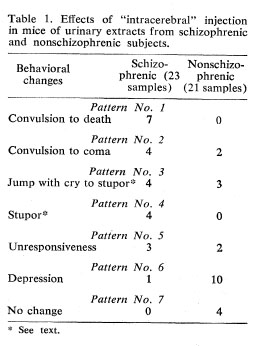
Fujita and Ging describe the toxicity of schizophrenic urine
Fujita and Ging were only cited five times, once by Chapman. And the Chapman article was cited once, by an book called “Brain Allergies: The Psycho-Nutrient Connection”. The search for signs of schizophrenia in the blood and urine seems to have yielded diminishing results over the years, whereas Chapman’s idea that these things were bacterial metabolites is still plausible, as there are still many studies hoping to link schizophrenia to infections. The infection in question is most often Chlamydia, the bacterium that causes urinary tract infections, or more recently Toxoplasma, the brain parasite popular with cat lovers (reviewed in Yolken et al [2009], Parasite Immunol 31(11): 706-715).
So the idea behind Chapman’s paper makes sense. And it contains a lot of data. However, the text shows worrying signs of crackpotism.
- Grandiosity: “My primary object throughout this research was to seek the cause of the obscure toxic states that accompany most chronic diseases.”
- Overambition: “…although time and space will not permit presentation of all the significant data, the statements which I shall make are based on careful and extensive experimentation, although this still does not preclude the possibility of error. Much of the detailed experimental data and its statistical analysis will be submitted to appropriate journals.” (this did not happen)
- Confusion: I think that when Fujita and Ging used the phrase “gummy substance”, they were referring to the entirety of the dried acetone extract of a urine sample, which was temporarily gummy because it had been processed in a certain way. They did not find a “gummy substance” in the urine. What they did find were unknown compounds that made spots on a Whatman chromatography paper.
Whereas Chapman talks about a “gummy substance” that makes up a particular alcohol fraction of the urine sample, that he observed in samples specifically from streptococcal UTI patients. - Trying to reduce things to simple physical laws: in this case, the redox potential of bodily fluids. Some of this looks logical and I don’t remember enough chemistry to judge. But I don’t know about statements like “A third example is the aggravation of colds following sexual indulgence. Loss of highly oxidized fluids causes a drop in the O/R potential of the body.”
- Auto-experimentation: “Therefore, I studied the effect of desiccated thyroid on the reducing power of the urine. I took 4 grain doses at frequent intervals and found that they improved, not only the oxidation of the urine, but the quat titer, rate of excretion, urates on refrigeration, and H-ion concentration. …Simultaneously with improvement in these findings there was dramatic improvement in general health.”
- Hobo legends: “The low O/R potential, particularly in severe cases, may provide an explanation for some unsolved phenomena. For example, “Bowery bums” are able to drink “smoke,” which is a water extract of shellac and consists mostly of crude methanol, and yet show no defect of vision.”
* * *
A full fourteen years after “Microbial origin of the gummy substance of Fujita and Ging”, and 48 years after the initial Chapman paper on Clostridium welchii, two other publications appeared. Both are in the 1976 issue of PDM: Physicians’ Drug Manual, which seems to be a book series published once each in 1973, 1974, and 1976. PubMed also lists 13 PDM articles from between 1958 and 1963. I don’t know what that means. And I don’t know how long the papers were either, since PubMed incomprehensibly cites them as PDM 1976 Jan-Dec;7(9-12)8(1-8):90-1 and PDM 1976 Jan-Dec;7(9-12)8(1-8):80-2. Probably short.
These papers (Acid-base and oxidation-reduction relationships and pH and eH relationships in the body) certainly seem to be by the same George H. Chapman. Based on the abstracts, there is a continuing fascination with redox potential and using urine as a readout for various health problems. In the second one, he also coins something called “Chapman’s Law”, another sign of crackpotism. Who knows what he was up to after the end of the Clinical Research Laboratory, but I’m sure he helped a lot of people with bacterial infections.
