A lot has been made nowadays about reproducibility, and how for some reason the most interesting scientific results are often the least reproducible. Evidently when there’s huge pressure to generate a certain graph containing certain data, either to give yourself a chance at fame and fortune or to give yourself a chance to have your lab and scientific career continue to exist, sometimes the graph does not represent the sort of objective reality that exists throughout space and time. This can be because of wishful thinking, because of selective use of the data that seems most solid, because of variables we never considered which later turn out to be crucial, who knows what else.
There have always been experiments where different labs get different results. Often we say that “in our hands,” we get Result X, but another laboratory gets Result Y, and we can say this without accusing anyone of malfeasance. It’s acceptable to get different results.
But nowadays, a scientist has no excuse when his contemporaries can’t even figure out how to replicate an experiment. A hundred years ago, it was more tricky. Even if you wrote and asked for a detailed protocol, it would probably involve terms that had no exact meaning. The topic under discussion today is the word “drop”.
* * *
In the December 1910 issue of the JAMA organ Archives of Internal Medicine, Drs. C. C. Bass and John A. Watkins wrote up (1) a new quick-and-easy test for typhoid that they had developed in the laboratories of Tulane University. The abstract is here, with subscription required to read the article. But this volume is old enough that it’s out of copyright and should be in Google Books. Though to be honest I can’t find it there and only found it at archive.org.
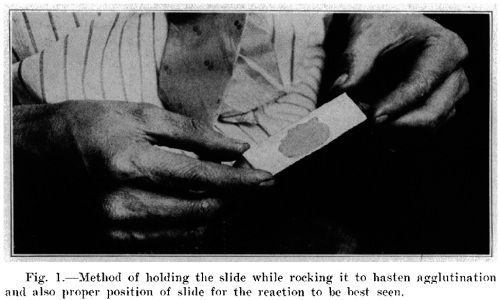
Over the ensuing years many doctors’ offices used it with more or less success, but as you might expect, many found they were unable to get results and went back to their old routine of sending samples to a clinical lab and waiting a day or two.Even though Bass and Watkins went to the trouble of including highly mundane photographs of things like proper slide-rocking procedure, people couldn’t figure out what exactly they were supposed to do. The text still contains phrases like “two to three drops of an equal number of bacilli units and agglutinin units sufficiently dilute to prevent rapid agglutination”. And “this one-quarter drop of blood is about the quantity we use in making blood slides in examinations for malaria, differential counts, etc.” The instructions are easy to understand, but really to communicate this sort of information you have to show people and let them practice it.
As a result, the 1910s saw some skeptical questions came in to the miscellaneous letters section of JAMA, sometimes with fairly impatient replies from the editors.
The editors of JAMA explain in detail the benefits of the Bass-Watkins test. (citation #2)
Following the usual routine of randomly skimming randomly selected old journals, I found a follow-up piece in the July 1918 New Orleans Medical and Surgical Journal (3) which goes into further detail trying to delineate concepts like “drop”. The author (presenter, rather, since this is the transcript of a talk which was followed by comments) is one of Bass and Watkins’s junior colleagues at Tulane, Foster M. Johns. Here’s what he says.
In the eight years that have elapsed since the publication of this article, this reaction has constantly grown in favor of the clinicians of the South, in spite of many improper lots of reagent supplied by private laboratories, my own included, as well as the various biological houses. During this time the test has been in constant use in the laboratories of clinical medicine with which I am connected, and it is with the belief that this reaction offers an easier, quicker and even more accurate reaction to not only the clinicians, but the trained laboratory worker as well, that I have prepared this discussion of a well-known test. During this time the few faults in technic and production brought out by continual use have been met and overcome, with the exception of a technic that will insure the uniform production of a stock suspension of typhoid bacilli that will keep well under the ordinary conventions of usage.
…
As simple as the technic sounds, there is often considerable difficulty in doing a simple thing. Taking up the test step by step, I will endeavor to point out the places where error may creep in. To begin with, an absolutely clean slide, freshly washed with soap and water to remove the grease and dust, most be used. Now, we require one-quarter of a drop of blood on the center of the slide. This is a quantity almost impossible to describe to one not accustomed to the routine making of proper blood smears, but practically it is easily approximated. Squeeze a quantity of blood out of a puncture on the finger or ear lobe that will not quite drop off, and then barely touch the slide to it. The quantity adhering to the slide will vary from one-quarter up to one-half of one drop. In either instance, for practical purposes, the end result will not be influenced… The actual dilution of the organisms will not be disturbed by either of the quantities of blood, as the blood is then spread roughly over the middle third of the slide and allowed to dry.
Now, one drop of plain water is added. Drops can vary enormously in size, and while, if the proportions in the test were carried out to suit, no harm would ensue, still, for working purposes, we need a full-sized drop. In this instance the standard drop is measured by preferably using the ordinary medicine dropper held almost parallel to the table, so that the drop collects on the side of the elongated glass tip of the dropper.
Full-sized drop? Quarter drop? A quarter drop is not a drop divided into fourths, but a drop that will not quite drop off? Or do you really mean a “finger or ear lobe that will not quite drop off”? In which case the real concern may be not typhoid, but leprosy.
Instead of all this … wouldn’t it be easier to measure volume in microliters?
I know nothing about the history of scientific equipment, but Wikipedia reports that there were no micropipettes until 1960. I don’t think there were syringes capable of measuring volumes on the level of a drop, either. And if there were such devices, they were far from disposable, and would need to be cleaned and dried between uses.
* * *
What is a drop anyway? And what was the smallest amount of volume that could be accurately measured a hundred years ago?
Again to the Wikipedia, which claims that today there is a medical definition of “drop” as 50 microliters. That means a quarter drop is 12.5 microliters, which sounds like about the right amount for a blood smear that you would quickly look at under a microscope.
Apothecaries traditionally were able to make much more precise measurements of weight than of volume. The common measurement of a “grain” is equal to 1/20 of a scruple, or 1/60 of a dram. And a dram is only 1/8 of an ounce, so there are 480 grains in an ounce, making a grain about 64 milligrams, under the old system where there were 12 ounces in a pound and a pound was about 1/3 of today’s kilogram.
Meanwhile, for liquids, people didn’t have too much trouble measuring in terms of scruples (slightly more than a cc or milliliter). But the minim, the volumetric equivalent of the grain, was only invented around the beginning of the 19th century, and required quite specialized equipment. Being the equivalent of a grain, the minim is about 64 microliters, or roughly… a drop. So it just made sense to refer to things in terms of drops. But when you factor in surface tension, temperature, the size of the vessel from which the drop is dropping… it’s always a judgment call. As the old saying goes, blood has a higher viscosity and specific density than water.
So those of us with access to space-age technology like micropipettes (and disposable anything) should count our blessings.
* * *
1. Bass CC, Watkins AA (1910). A quick macroscopic typhoid agglutination test. Arch Inter Med VI(6):717-729.
2. from “Miscellany”, September 5th (1914). Value of von Pirquet reaction in adults / Reliability of Bass-Watkins test. J Am Med Assoc LXIII(10):883.
3. Johns FM (1918). The Bass-Watkins agglutination test for typhoid. New Orleans Med Surg J LXXI(1):22-27.






